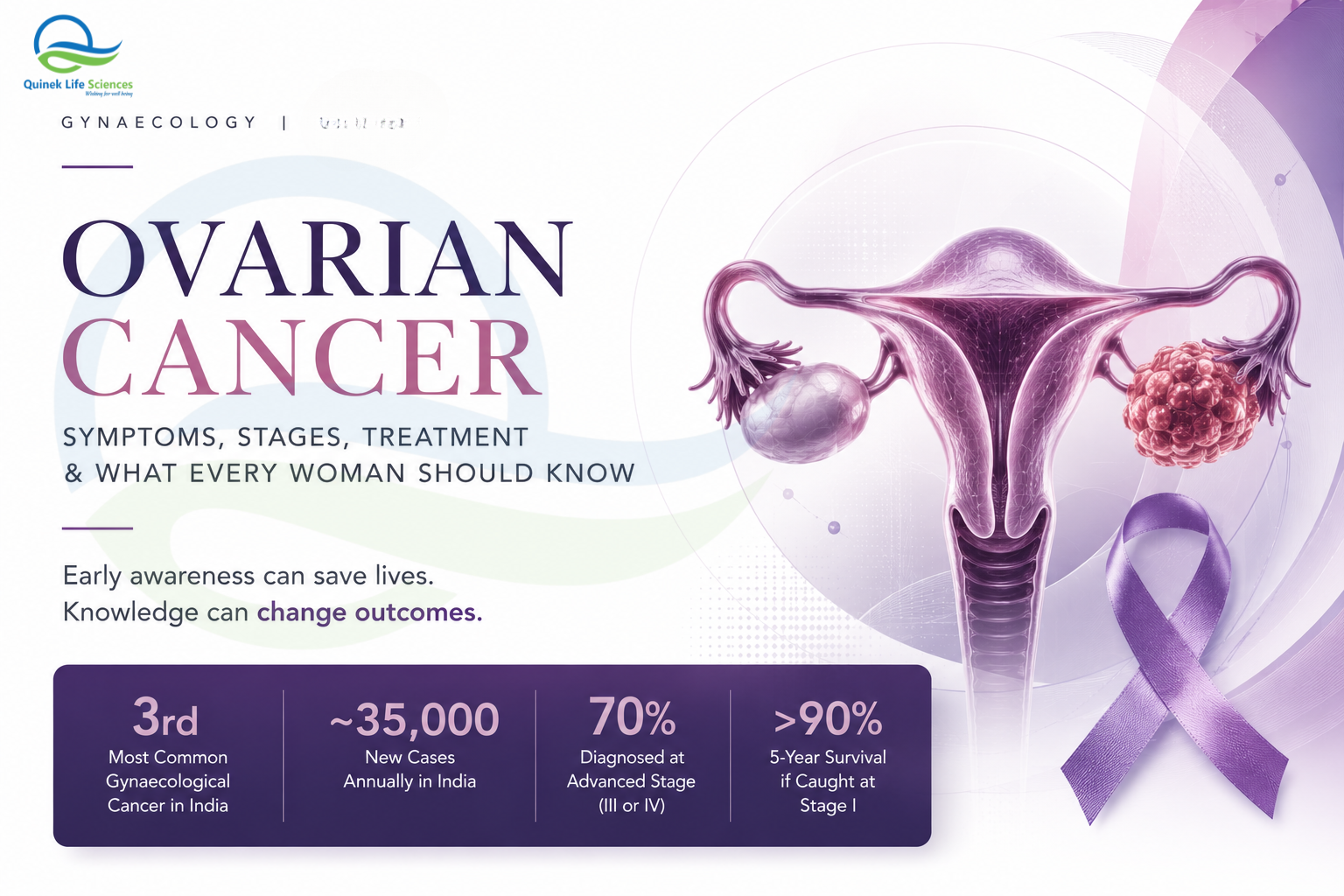
3rd
Most Common Gynaecological Cancer in India
~35,000
New Cases Annually in India
70%
Diagnosed at Advanced Stage (III or IV)
>90%
5-Year Survival if Caught at Stage I
Ovarian cancer has earned a grim reputation — not because it is the most common gynaecological cancer, but because it is the most silent. Unlike cervical cancer, there is no reliable screening test. Unlike breast cancer, there is no widely practised self-examination. The ovaries sit deep in the pelvis, and the symptoms of early ovarian cancer — bloating, mild abdominal discomfort, a change in urinary habits — are so non-specific that they are dismissed for months, sometimes years, before a diagnosis is made.
By the time most women in India are diagnosed with ovarian cancer, the disease has already spread beyond the ovary. This is not inevitable — it is a consequence of low awareness, delayed presentation and a healthcare system that has not yet built the same level of public education around ovarian cancer that it has around cervical and breast cancer.
This article is for women who want to understand the warning signs, for families navigating a new diagnosis, and for general practitioners and gynaecologists who want a comprehensive clinical reference. The goal is simple: earlier awareness, earlier presentation, better outcomes.
IN THIS ARTICLE
- What Is Ovarian Cancer?
- Types of Ovarian Cancer
- Symptoms — The Signs Most Women Miss
- Risk Factors — Who Is at Higher Risk?
- Stages of Ovarian Cancer
- How Ovarian Cancer Is Diagnosed
- Treatment Options — What the Evidence Says
- Can Ovarian Cancer Be Prevented?
- Frequently Asked Questions
- Quinek Life Sciences — Gynaecology Pharmaceutical Support
What Is Ovarian Cancer?
Ovarian cancer is a malignant tumour that originates in the ovaries — the two small, almond-shaped organs in the female pelvis that produce eggs and the hormones oestrogen and progesterone. When cells in or around the ovary begin to grow abnormally and uncontrollably, they form a tumour that, if malignant, can invade surrounding tissue and spread to other parts of the body.
What makes ovarian cancer particularly dangerous is the combination of its deep pelvic location, its non-specific early symptoms and the absence of a reliable population-level screening tool. The CA-125 blood test and pelvic ultrasound are used in clinical evaluation, but neither has been validated as a mass screening tool with sufficient sensitivity and specificity to change outcomes at a population level.
INDIA — OVARIAN CANCER BURDEN
Approximately 35,000 new cases annually in India · Source: NCBI — Ovarian Cancer in India
Ovarian cancer is the 3rd most common gynaecological cancer in India after cervical and uterine cancer
Over 70% of cases are diagnosed at Stage III or IV — when prognosis is significantly worse · Source: WHO Cancer Fact Sheet
Types of Ovarian Cancer
Ovarian cancer is not a single disease — it is a group of distinct malignancies that differ in their cell of origin, behaviour, response to treatment and prognosis. Understanding the type of ovarian cancer matters clinically because treatment protocols, chemotherapy regimens and targeted therapy options differ significantly.
Epithelial Ovarian Cancer
The most common type — accounting for 85–90% of all ovarian cancers. Arises from the epithelial cells covering the surface of the ovary or fallopian tube. Includes high-grade serous carcinoma (the most common and aggressive subtype), endometrioid, clear cell and mucinous carcinomas.
Germ Cell Tumours
Arise from the egg-producing cells of the ovary. More common in younger women and girls. Include dysgerminoma, teratoma and yolk sac tumours. Generally more responsive to chemotherapy than epithelial types — prognosis is often better even at advanced stages.
Sex Cord-Stromal Tumours
Arise from the connective tissue cells that hold the ovary together and produce hormones. Include granulosa cell tumours and Sertoli-Leydig tumours. May cause hormonal symptoms (abnormal bleeding, virilisation). Tend to grow slowly and are often diagnosed at an earlier stage.
Symptoms — The Signs Most Women Miss
The most dangerous aspect of ovarian cancer is not its aggressiveness — it is its subtlety. Early ovarian cancer is often completely asymptomatic. When symptoms do appear, they tend to be vague, intermittent and easily attributed to more common and benign conditions like irritable bowel syndrome, UTIs or general digestive issues.
The key clinical insight is persistence and combination. Any one of the symptoms below, appearing occasionally, is unlikely to signal ovarian cancer. But when two or more symptoms occur together, frequently, for more than two to three weeks, and represent a change from the person’s normal pattern — that warrants gynaecological evaluation.
THE TWO-WEEK RULE
If you experience any combination of the above symptoms — persistent (occurring more than 12 times per month), representing a change from your normal — for more than two weeks, see a gynaecologist. Do not wait. Early detection is the single most powerful determinant of ovarian cancer survival. Reference: Cancer Research UK — Ovarian Cancer Symptoms
Risk Factors — Who Is at Higher Risk?
No single risk factor causes ovarian cancer — but a combination of genetic, hormonal, reproductive and lifestyle factors can significantly elevate a woman’s lifetime risk. Understanding these risk factors helps identify women who may benefit from enhanced surveillance or risk-reduction strategies.
Stages of Ovarian Cancer
Ovarian cancer is staged according to the FIGO (International Federation of Gynaecology and Obstetrics) staging system. Stage at diagnosis is the single most important prognostic factor — which is why early detection matters so enormously.
How Ovarian Cancer Is Diagnosed
There is no reliable single screening test for ovarian cancer in the general population. Diagnosis is typically triggered by symptoms, a pelvic mass found on examination or ultrasound, or incidental finding during imaging for another reason. The diagnostic workup then involves a combination of investigations to confirm the diagnosis, characterise the tumour and stage the disease.
Transvaginal Ultrasound (TVUS)
The first-line imaging investigation for suspected ovarian pathology. It evaluates the size, morphology and internal characteristics of ovarian masses — solid vs cystic, presence of septations, papillary projections and vascularity. The IOTA (International Ovarian Tumour Analysis) criteria are used to risk-stratify ovarian lesions on ultrasound.
CA-125 Blood Test
CA-125 is a tumour marker elevated in many cases of epithelial ovarian cancer — but it is not diagnostic. It can be elevated in benign conditions (endometriosis, fibroids, pelvic inflammatory disease, even pregnancy) and may be normal in early-stage ovarian cancer. It is most useful when used in combination with ultrasound (the Risk of Malignancy Index — RMI) and for monitoring treatment response in known cases.
CT / MRI of Abdomen and Pelvis
Essential for staging — characterising the extent of disease, assessing lymph node involvement, evaluating peritoneal spread and identifying distant metastases. CT is the workhorse of ovarian cancer staging. MRI provides superior soft tissue detail for local pelvic assessment.
Histopathology — The Definitive Diagnosis
Definitive diagnosis requires tissue — either from surgical excision of the ovarian mass, laparoscopic biopsy or, in cases of advanced disease with ascites, cytological examination of ascitic fluid. The histopathological report confirms the diagnosis, identifies the tumour type and subtype, and guides treatment planning.
Treatment Options — What the Evidence Says
Ovarian cancer treatment is multimodal — combining surgery and chemotherapy as the backbone, with targeted therapies increasingly available for specific molecular subtypes. Treatment planning should be done by a multidisciplinary team at a gynaecological oncology centre.
Surgery — Cytoreduction / Debulking
Surgery is the cornerstone of ovarian cancer treatment in most stages. The goal of primary surgery is complete cytoreduction — removing all visible tumour — because the completeness of surgical debulking is one of the strongest prognostic factors. Standard surgery includes total hysterectomy, bilateral salpingo-oophorectomy, omentectomy and removal of all visible peritoneal disease. In younger women with early-stage disease wishing to preserve fertility, fertility-sparing surgery may be possible in selected cases.
Chemotherapy — Platinum-Based Regimens
Carboplatin and paclitaxel (the platinum-taxane doublet) is the standard first-line chemotherapy for epithelial ovarian cancer. It is administered intravenously, typically for 6 cycles. The majority of patients respond to first-line platinum-based chemotherapy — but relapse is common in advanced disease, and managing relapse is one of the central challenges in ovarian cancer care. Reference: NEJM — Standard Chemotherapy in Ovarian Cancer
PARP Inhibitors — Targeted Therapy
For women with BRCA1/2 mutations or homologous recombination deficiency, PARP inhibitors (olaparib, niraparib, rucaparib) have transformed the maintenance treatment landscape — significantly prolonging progression-free survival after platinum-based chemotherapy. BRCA testing is now recommended for all women with high-grade serous ovarian cancer. Reference: NEJM — PARP Inhibitors in Ovarian Cancer
Bevacizumab — Anti-Angiogenic Therapy
Bevacizumab, an anti-VEGF monoclonal antibody, is approved in combination with chemotherapy and as maintenance therapy in advanced ovarian cancer. It has demonstrated improvements in progression-free survival, particularly in high-risk Stage III/IV disease and platinum-sensitive relapse.
IMPORTANT FOR PATIENTS
Treatment decisions for ovarian cancer should always be made by a gynaecological oncologist in a multidisciplinary setting. India has an increasing number of dedicated gynaecological oncology centres — seek referral to one at the earliest opportunity after diagnosis. The International Gynecologic Cancer Society (IGCS) provides global treatment guidelines that are applied in Indian specialist centres.
Can Ovarian Cancer Be Prevented?
There is no guaranteed way to prevent ovarian cancer — but there are evidence-based strategies that meaningfully reduce risk, particularly in women at elevated genetic risk.
Oral Contraceptives
5+ years of OCP use reduces lifetime ovarian cancer risk by approximately 50%. The protective effect persists for decades after stopping. This is one of the most robust protective associations in cancer epidemiology.
Risk-Reducing Surgery (RRSO)
For women with BRCA1/2 mutations, risk-reducing bilateral salpingo-oophorectomy reduces ovarian cancer risk by over 85% and significantly reduces breast cancer mortality. Typically recommended between age 35–40 after childbearing is complete.
BRCA Genetic Testing
Women with a strong family history of ovarian or breast cancer should discuss BRCA genetic testing with a specialist. Knowing your BRCA status enables proactive risk management — including enhanced surveillance and risk-reduction surgery.
Breastfeeding & Parity
Each full-term pregnancy and period of breastfeeding reduces ovarian cancer risk modestly — likely by reducing the number of lifetime ovulatory cycles and associated hormonal fluctuations.
Frequently Asked Questions
Q. Is ovarian cancer hereditary?
Approximately 15–20% of ovarian cancers are hereditary — most commonly linked to BRCA1 or BRCA2 mutations, or Lynch syndrome. The majority of ovarian cancers are sporadic, occurring without a clear genetic cause. If you have a first-degree relative with ovarian or breast cancer, discuss genetic counselling with your gynaecologist.
Q. Can an ovarian cyst become cancer?
Most ovarian cysts are benign — particularly in premenopausal women. Simple, unilocular cysts are almost never malignant. Complex cysts with solid components, internal papillary projections or irregular septations carry a higher risk and require evaluation by a specialist. Post-menopausal cysts — even simple ones — warrant more careful surveillance.
Q. Is CA-125 a reliable screening test for ovarian cancer?
No — not for general population screening. CA-125 lacks sufficient sensitivity and specificity to be used as a standalone screening tool. It can be elevated in benign conditions and may be normal in early ovarian cancer. It is most useful for monitoring treatment response and detecting recurrence in known ovarian cancer cases.
Q. Can ovarian cancer be treated successfully?
Yes — particularly when caught early. Stage I ovarian cancer has a 5-year survival rate exceeding 90%. Even in advanced stages, modern chemotherapy, targeted therapies and maintenance treatment have significantly improved outcomes over the past decade. Treatment is always possible; outcomes depend heavily on stage, tumour type and access to specialist care.
Q. At what age should women start worrying about ovarian cancer?
Ovarian cancer can occur at any age, but risk increases significantly after 50. Germ cell tumours are more common in younger women and girls. Any woman — at any age — who develops persistent, unexplained abdominal or pelvic symptoms should see a gynaecologist. Age is a risk factor but not a prerequisite for concern.
Quinek Life Sciences — Gynaecology Pharmaceutical Support
Quinek Life Sciences is a WHO-GMP, GLP, ISO, DCGI and FSSAI certified specialty pharmaceutical company with a comprehensive gynaecology portfolio — covering hormonal therapy, progesterone supplementation, ovulation induction, endometriosis management, vaginal infection care, nutritional support in pregnancy and more.
While ovarian cancer management requires specialist oncology care, supportive pharmaceutical management — hormonal optimisation, nutritional support during chemotherapy, management of treatment-related symptoms — remains an important part of the overall care pathway. Quinek’s certified gynaecology portfolio supports gynaecologists across this full spectrum of women’s health care.
“Over 90% of ovarian cancers diagnosed at Stage I are survivable. Awareness is the earliest intervention.”
Quinek Life Sciences — WHO-GMP Certified Gynaecology Pharmaceutical Company, India
References & Further Reading
- NCBI — Ovarian Cancer Burden in India
- WHO — Cancer Fact Sheet, 2023
- FIGO — Staging of Gynaecological Cancers
- NEJM — Chemotherapy in Advanced Ovarian Cancer
- NEJM — PARP Inhibitors in Ovarian Cancer
- Cancer Research UK — Ovarian Cancer Symptoms
- International Gynecologic Cancer Society — Treatment Guidelines
- Quinek Life Sciences — Gynaecology Segment
This article is for educational and awareness purposes only. It does not constitute medical advice. Always consult a qualified gynaecologist or oncologist for diagnosis and treatment. If you have symptoms of concern, seek medical evaluation promptly.